
You notice blood on the toilet paper, or a tender lump that makes sitting miserable, and the first question is usually simple. Is this an internal hemorrhoid or an external one?
That difference matters because the location changes what you feel, what usually helps, and when you should get checked quickly. Some hemorrhoids mainly bleed. Others mainly hurt. Some stay hidden inside the anal canal. Others can be felt on the outside. Mixed hemorrhoids can do both.
For adults dealing with constipation, pregnancy-related pressure, long hours of sitting, or bowel changes after GLP-1 medications, this confusion is common.
We understand that comfort is important during the healing process, which is why individuals often seek supportive methods to alleviate discomfort and enhance recovery, in addition to medical treatment.
Understanding Your Discomfort
Examination of the anal canal’s anatomy typically occurs only when a problem arises. What patients notice first is discomfort, spotting, swelling, itching, or pain with bowel movements.
That symptom alone doesn’t tell the whole story. The difference between internal and external hemorrhoids starts with where they form, and that location shapes nearly everything else.
External hemorrhoids sit in pain-sensitive tissue, so they tend to announce themselves fast. Internal hemorrhoids sit higher up, where the lining isn’t sensitive to pain in the same way, so they often show up as bleeding or prolapse instead of sharp pain.
Many adults assume any hemorrhoid should hurt. That’s one of the main reasons internal hemorrhoids are so confusing.
A practical way to think about it is this:
-
If the main issue is pain or a tender lump outside, an external hemorrhoid is more likely.
-
If the main issue is bright red bleeding with little or no pain, an internal hemorrhoid moves higher on the list.
-
If symptoms change from one day to the next, you may be dealing with a mixed pattern or another anorectal condition that deserves an exam.
We want readers to leave this topic less anxious and more precise. Not every hemorrhoid needs a procedure. Not every painful lump is dangerous. But not every bleeding episode should be shrugged off, either.
Anatomy 101 Where Hemorrhoids Form
The key landmark is the dentate line. Think of it as a dividing line inside the anal canal. Tissue above and below that line behaves differently.
Internal hemorrhoids
Internal hemorrhoids form above the dentate line. They are covered by rectal mucosa, which doesn’t sense pain the way skin does. That’s why internal hemorrhoids commonly bleed without causing much pain.
They are also graded by prolapse. Grade I stays inside. Grade II comes out with straining and goes back in on its own. Grade III needs manual reduction. Grade IV stays out and can’t be reduced. The anatomy and grading framework are summarized in the NCBI review on hemorrhoids at https://www.ncbi.nlm.nih.gov/books/NBK500009/.
External hemorrhoids
External hemorrhoids form below the dentate line. They are covered by anoderm and perianal skin, which are rich in nerve endings that sense pain, stretch, and temperature. That is why a relatively small external hemorrhoid can feel disproportionately uncomfortable.
This outer location also explains why people can often see or feel external hemorrhoids more easily. They may seem like a swollen bump, soft tissue fullness, or, when thrombosed, a firmer painful lump.
Practical rule: If tissue is in skin-level territory, symptoms tend to be more about pain, tenderness, and swelling. If it’s higher inside the canal, symptoms are more often about bleeding or prolapse.
Hemorrhoids are common enough that most adults will encounter them at some point. Their incidence peaks between 45 and 65 years, and three out of four adults experience hemorrhoids during life, according to the same NCBI review linked above.
Supportive bowel and circulation habits matter because pressure and venous congestion contribute to flare-ups. For a patient-friendly look at that relationship, see https://bummed.co/the-gut-vein-connection-how-diosmin-supports-circulation-and-hemorrhoid-health/.
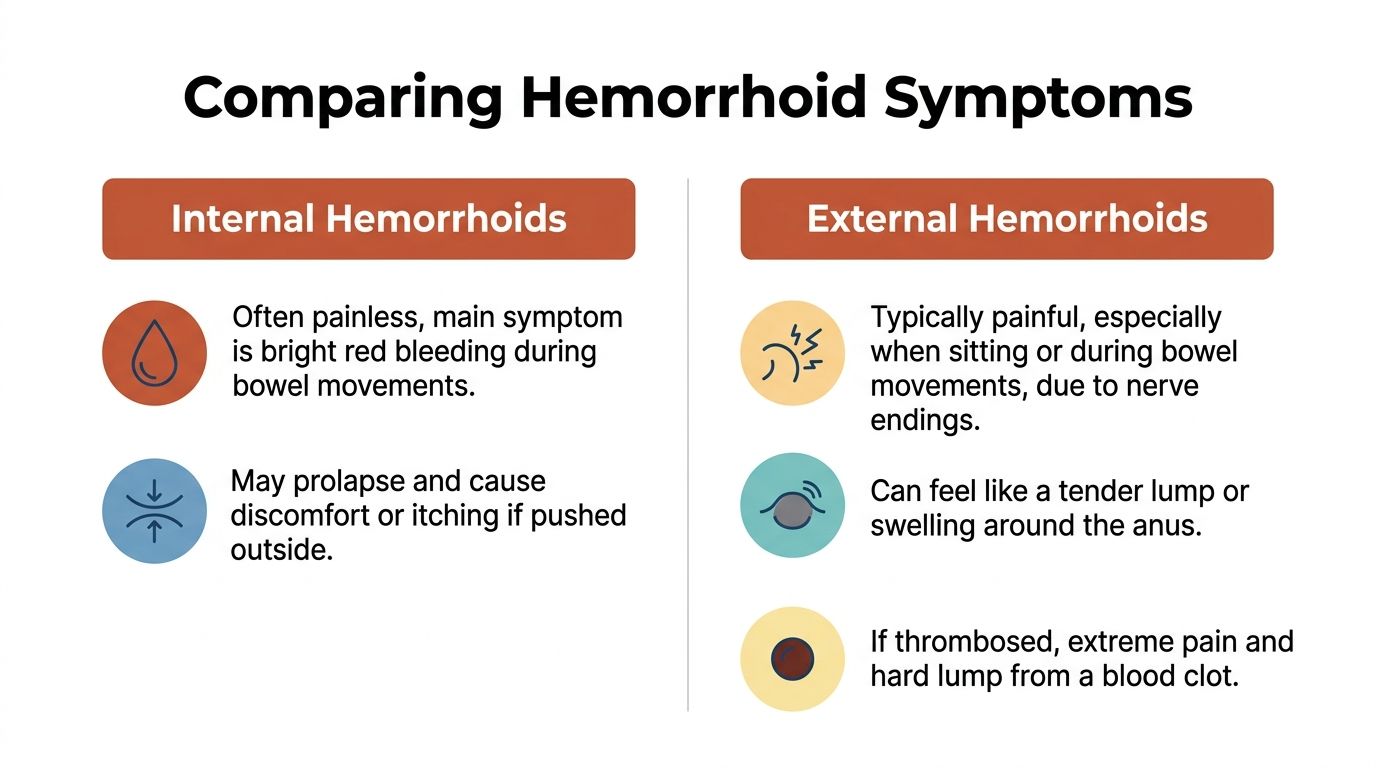
Comparing Symptoms Pain vs Bleeding
The fastest way to understand the difference between internal and external hemorrhoids is to compare what people feel.
| Feature | Internal Hemorrhoids | External Hemorrhoids |
|---|---|---|
| Location | Inside the anal canal, above the dentate line | Around the anus, below the dentate line |
| Pain | Usually little or no pain unless prolapsed | Often painful because the tissue is richly innervated |
| Bleeding | More likely to cause bright red rectal bleeding | May bleed, but pain and swelling are often more prominent |
| Appearance | Usually not visible unless prolapsed | Often visible or palpable as a lump or swelling |
| Exam | Often needs digital rectal exam or anoscopy | Often identified on visual exam or palpation |
| Common trouble spot | Prolapse and bleeding | Thrombosis, swelling, tenderness |
Pain and pressure
External hemorrhoids are usually the painful ones. The reason is straightforward. They sit in tissue with dense sensory nerves.
When an external hemorrhoid becomes thrombosed, meaning a clot forms inside it, the pressure on the surrounding skin can cause significant pain. The NCBI review notes that pain from sudden distension by clotted blood can last 5 to 12 days at https://www.ncbi.nlm.nih.gov/books/NBK500009/.
Internal hemorrhoids are different. They are typically painless unless they prolapse or become irritated enough to create pressure, mucus, or hygiene issues.
Bleeding patterns
Bright red blood with bowel movements points more often toward an internal source. Cleveland Clinic notes that internal hemorrhoids commonly present with painless bright red rectal bleeding, while external hemorrhoids are more associated with pain, itching, swelling, and thrombosis at https://consultqd.clevelandclinic.org/hemorrhoids-the-definitive-guide-to-medical-and-surgical-treatment.
That doesn’t mean every episode of rectal bleeding is “just hemorrhoids.” It means hemorrhoids are one possible explanation, especially if the blood is bright red and appears on the stool or toilet paper.
If bleeding is your main symptom, this guide on https://bummed.co/blood-when-you-wipe-here-is-what-doctors-need-you-to-know/ helps frame what providers look for.
Appearance and feel
External hemorrhoids are often easier to identify at home because they can be seen or felt. They may be skin-colored. If thrombosed, they often look darker or purplish and feel firm and tender.
Internal hemorrhoids are usually not visible unless they prolapse. When they do, they may appear pink or mucosa-colored, more like tissue from inside the mouth than outside skin. Mixed hemorrhoids can have both internal and external components, which is one reason self-diagnosis can be tricky.
A few practical clues help:
-
Visible outside bump with soreness: more consistent with an external hemorrhoid.
-
Tissue that comes out during straining: raises concern for a prolapsing internal hemorrhoid.
-
Hard, very tender purple lump: often suggests a thrombosed external hemorrhoid.
-
Spotting without much discomfort: often fits the internal pattern better.
If you can describe whether the problem is mainly bleeding, mainly pain, or mainly prolapse, your provider can usually narrow the possibilities quickly.
Common Causes and Modern Risk Factors
Hemorrhoids don’t appear at random. They usually develop when pressure repeatedly builds in the veins and supporting tissue around the anal canal.
The usual drivers
Chronic straining remains one of the biggest contributors. Constipation, hard stools, prolonged time on the toilet, and repeated pressure during bowel movements can all aggravate hemorrhoidal tissue.
Avoiding straining is especially important for preventing prolapse. Fiber also matters. Cleveland Clinic’s hemorrhoid review recommends 25 to 30 g/day of fiber to help prevent flare-ups and notes that adding it gradually can help avoid diarrhea at https://consultqd.clevelandclinic.org/hemorrhoids-the-definitive-guide-to-medical-and-surgical-treatment.
Pregnancy and postpartum pressure
Pregnancy is a major risk period because pressure inside the abdomen rises, bowel habits often change, and delivery itself can stress the hemorrhoidal veins. The NCBI review reports that prevalence in pregnancy reaches up to 35%, with straining, hard stools, and childbirth contributing to venous engorgement, bleeding, thrombosis, or prolapse at https://www.ncbi.nlm.nih.gov/books/NBK500009/.
That pattern is familiar in practice. Patients often describe a flare that starts late in pregnancy, after delivery, or during a stretch of constipation while recovering postpartum.
GLP-1 medications and constipation
A newer issue is bowel slowing with GLP-1 medications such as semaglutide. The practical concern isn’t the medication itself. It’s what happens if constipation and straining follow.
Internal hemorrhoids are graded 1 to 4 by prolapse and that progression is linked to chronic straining. Constipation can affect 20 to 40% of users on GLP-1 medications like semaglutide, which helps explain why some adults notice new hemorrhoid symptoms after starting these drugs.
This doesn’t mean anyone on a GLP-1 will develop hemorrhoids. It means bowel management becomes more important. If stools are getting harder, less frequent, or more difficult to pass, that’s the moment to intervene early rather than waiting for a painful flare.
The modern pattern we see most often is simple. Constipation changes first. Hemorrhoid symptoms follow.
Your Treatment Options From Home Care to Procedures
For many adults, the first step is the same whether the hemorrhoid is internal or external. Reduce pressure. Calm inflammation. Make bowel movements easier.

What often helps first
Conservative care works best when symptoms are still early.
-
Softer stools: Fiber and hydration reduce the repeated friction and straining that keep hemorrhoids irritated.
-
Warm soaks: Sitz baths can be particularly helpful for external swelling and spasm. Cleveland Clinic notes they can reduce external swelling by 50% in 48 hours at https://consultqd.clevelandclinic.org/hemorrhoids-the-definitive-guide-to-medical-and-surgical-treatment.
-
Topical support: Prescription compounded creams may help address pain, irritation, inflammation, or spasm depending on the formulation. Bummed is the only telehealth platform to prescribe custom compounded creams for hemorrhoids and fissures.
-
Less mechanical pressure: Don’t sit and strain. Don’t linger on the toilet when nothing is happening.
Heat can also help with muscle relaxation and comfort. For people curious about broader pain-relief principles, this overview of remarkable benefits of heat therapy gives useful context.
If you want a practical home-first guide, https://bummed.co/how-to-get-rid-of-hemorrhoids-fast/ covers common relief steps clearly.
Treatment often fails for one boring reason. The stool stays hard, so the tissue gets re-injured every day.
When procedures make sense
Procedural treatment depends on the type of hemorrhoid.
For symptomatic internal hemorrhoids, office-based procedures are often effective. Cleveland Clinic reports that rubber band ligation has a success rate of over 80% for grades I to III internal hemorrhoids, and that post-procedure pain occurs in 5 to 10% of cases: https://consultqd.clevelandclinic.org/hemorrhoids-the-definitive-guide-to-medical-and-surgical-treatment
Rubber band ligation works because it cuts off blood supply to the internal hemorrhoid. That causes the tissue to shrink. It is not used for external hemorrhoids.
For small internal hemorrhoids, providers may also consider infrared coagulation or sclerotherapy. Those approaches are generally aimed at internal tissue that bleeds or prolapses but doesn’t need full surgery.
For a thrombosed external hemorrhoid, the trade-off is speed versus watchful care. If the pain is severe and the clot is fresh, excision under local anesthesia can bring rapid relief. Cleveland Clinic notes that excision can provide 95% pain relief within 24 to 48 hours for thrombosed external hemorrhoids at the same Cleveland Clinic URL cited above.
This is one of the clearest differences in treatment strategy:
-
Internal hemorrhoids: often respond to banding or other office procedures.
-
External thrombosed hemorrhoids: may need clot-focused evaluation, and banding isn’t appropriate.
When to Seek Urgent Medical Care
Most hemorrhoids are uncomfortable, not dangerous. The problem is that a few symptoms overlap with conditions that shouldn’t wait.

Red flags you shouldn’t ignore
Get prompt medical evaluation if you have any of the following:
-
Heavy or ongoing rectal bleeding: especially if it doesn’t settle or keeps recurring.
-
Black or maroon stools: hemorrhoids usually cause bright red blood, not dark stool.
-
Severe pain that escalates quickly: especially with a new lump.
-
Fever or feeling systemically unwell: hemorrhoids alone don’t usually cause this.
-
A sudden major change in bowel habits plus rectal bleeding: that combination deserves a proper workup.
-
Dizziness, weakness, or faintness with bleeding: don’t manage that at home.
Telehealth can be a good first step for many hemorrhoid questions. It isn’t the right setting for clear emergency symptoms.
Why thrombosed external hemorrhoids need prompt attention
A thrombosed external hemorrhoid is a blood clot in an external vein. It often causes a painful, purple lump and tends to hit hardest early. The MWHTC review notes that peak pain occurs at 48 to 72 hours, and that early conservative treatment with topicals, like those from Bummed, and sitz baths can resolve up to 80% of cases without surgery. It also notes that a provider can decide whether thrombectomy is needed: https://www.mwhtc-stl.com/blog/understanding-the-difference-between-external-and-internal-hemorrhoids
That timing matters. If you’re in intense pain and a lump appeared quickly, getting evaluated sooner can make relief easier and faster.
Sudden severe pain with a purple lump is not the moment to “wait and see” for a week.
Frequently Asked Questions About Hemorrhoids
Can you have both internal and external hemorrhoids at the same time
Yes. Mixed hemorrhoids happen. In those cases, people may report both bleeding and an outside lump or tenderness. The initial home treatment is often similar, but procedural options differ because external hemorrhoids aren’t treated the same way as internal ones.
Do internal hemorrhoids always bleed
No. Some internal hemorrhoids don’t cause noticeable symptoms at all. Others mainly cause prolapse, mucus, or a sense of pressure. When they do bleed, the bleeding is often bright red and not especially painful.
Are external hemorrhoids always painful
No. Some are more annoying than painful and may feel like swelling, itching, or a soft tag. Pain becomes much more prominent when an external hemorrhoid thromboses or gets significantly irritated.
Can telehealth be a good first step
Often, yes. Telehealth can work well for common hemorrhoid symptoms, especially when the question is whether you can start conservative treatment safely, whether a prescription topical may help, or whether the symptom pattern sounds more like hemorrhoids than another anorectal issue.
It’s less appropriate when bleeding is heavy, pain is severe and escalating, or you have red-flag symptoms that need in-person evaluation.
What helps prevent flare-ups
A few habits matter more than people expect:
-
Keep stools easy to pass: constipation is one of the most common drivers.
-
Stop straining: repeated bearing down worsens both bleeding and prolapse risk.
-
Respond early: treat bowel changes before they become a week of hard stools.
-
Limit long toilet sessions: pressure and friction add up.
-
Pay attention to triggers: pregnancy, travel, medication changes, and GLP-1-related constipation are common setup factors.
The best prevention plan is usually boring and effective. Keep the stool soft, keep the bathroom time short, and avoid repetitive strain.
Important Medical Disclaimers
Bummed content is for general education and should never replace professional medical advice that considers your individual health. If you think you’re experiencing a medical emergency, call 911 or head to the nearest emergency department.
Prescription products require an online consultation with a physician who will determine if a prescription is appropriate.
If you’re dealing with hemorrhoid symptoms and want discreet, specialist-informed care, Bummed offers online evaluation for anorectal concerns, including custom, surgeon-formulated prescription creams that may be prescribed if appropriate.