
A fissure often starts with one bad bowel movement, then turns into a problem that shapes your whole day. You may dread using the bathroom, sit differently at work, and keep trying over-the-counter creams that soothe for an hour but never seem to fix the actual tear.
That pattern is common. The best cream for anus fissure usually isn’t the one that numbs the area the most. It’s the one that helps the tissue heal by relaxing the internal anal sphincter, improving blood flow, and stopping the cycle that keeps re-tearing the skin.
What Is an Anal Fissure and Why Won't It Heal
An anal fissure is a small tear in the lining of the anal canal. Small doesn’t mean mild. This tissue is highly sensitive, so even a short tear can cause sharp pain, burning, and bleeding with bowel movements.
What makes fissures so frustrating is that they don’t behave like a simple paper cut. They get trapped in a repeat injury cycle.

The pain spasm blood flow cycle
Here’s what usually happens:
A hard stool or straining causes a tear.
The tear triggers pain.
Pain makes the internal anal sphincter clamp down.
That spasm reduces blood flow to the fissure.
Poor blood flow prevents healing.
The next bowel movement reopens the tear.
It's like trying to heal a cracked lip while stretching it open several times a day. The tissue never gets enough rest or circulation to close.
Practical rule: If a treatment only dulls pain but doesn’t relax the sphincter, it usually won’t solve a chronic fissure.
Why constipation keeps restarting the problem
Constipation is one of the biggest drivers of this cycle. Large, dry stool creates the initial trauma, and repeated straining keeps the wound active. That’s why fissure care always includes stool management, not just a cream.
If bleeding is part of what brought you here, our guide on constipation and rectal bleeding explains when constipation is the likely trigger and when it deserves a closer medical look.
Acute versus chronic fissures
Some fissures heal quickly once the stool softens and irritation settles down. Others become chronic, meaning the area stays inflamed and the muscle underneath remains tight. In that setting, the issue isn’t only the surface tear. It’s the muscle spasm underneath it.
That’s why the best cream for anus fissure is usually a prescription treatment aimed at the muscle, not just the skin.
Why Over-the-Counter Creams Don't Work for Fissures
Many adults assume a fissure should respond to the same products used for hemorrhoids. That’s understandable, but it’s usually the wrong match.
Most over-the-counter creams are built to do one of three things: numb the area, reduce irritation, or protect the skin surface. Those effects can help symptoms, but they don’t address the core problem in a fissure, which is internal sphincter spasm with poor blood flow.
What OTC products can do
Some common ingredient types can offer short-term comfort:
Local anesthetics can numb burning and stinging.
Protectants can reduce friction during bowel movements.
Mild anti-inflammatory ingredients can calm itching or irritation.
Barrier ointments can shield already irritated skin.
That can make a person feel better temporarily. It can also create the impression that healing has started when the fissure is still mechanically stuck open.
What OTC products can’t do
They generally do not chemically relax the internal anal sphincter in the way prescription fissure medications do. And if the muscle stays tight, blood flow stays limited.
Temporary relief isn’t the same as healing. A fissure can hurt less for a few hours and still remain unhealed.
This is why people often say, “I tried every cream and nothing worked.” In many cases, they tried products that were never designed to fix a fissure’s underlying physiology.
Why hydrocortisone isn’t usually the answer
Hydrocortisone can reduce irritation, but fissures are not primarily a steroid-deficiency problem. They’re a blood flow and muscle spasm problem. That distinction matters. A cream that reduces redness may still leave the fissure trapped in the same cycle.
If a tear keeps hurting with bowel movements, keeps bleeding, or keeps returning after brief improvement, it’s time to stop guessing and move to a treatment that targets the reason it won’t heal.
Prescription Creams The Medical Gold Standard
A chronic fissure usually persists because the internal anal sphincter stays in spasm. That spasm keeps pressure high and blood flow low at the edge of the tear. In practice, that is the problem prescription creams are designed to treat.
For chronic fissures, the standard medical approach is chemical sphincterotomy. The term sounds technical, but the idea is simple. Instead of cutting the muscle, medication relaxes it enough to reduce pressure and let oxygen-rich blood reach the wound so it can heal.
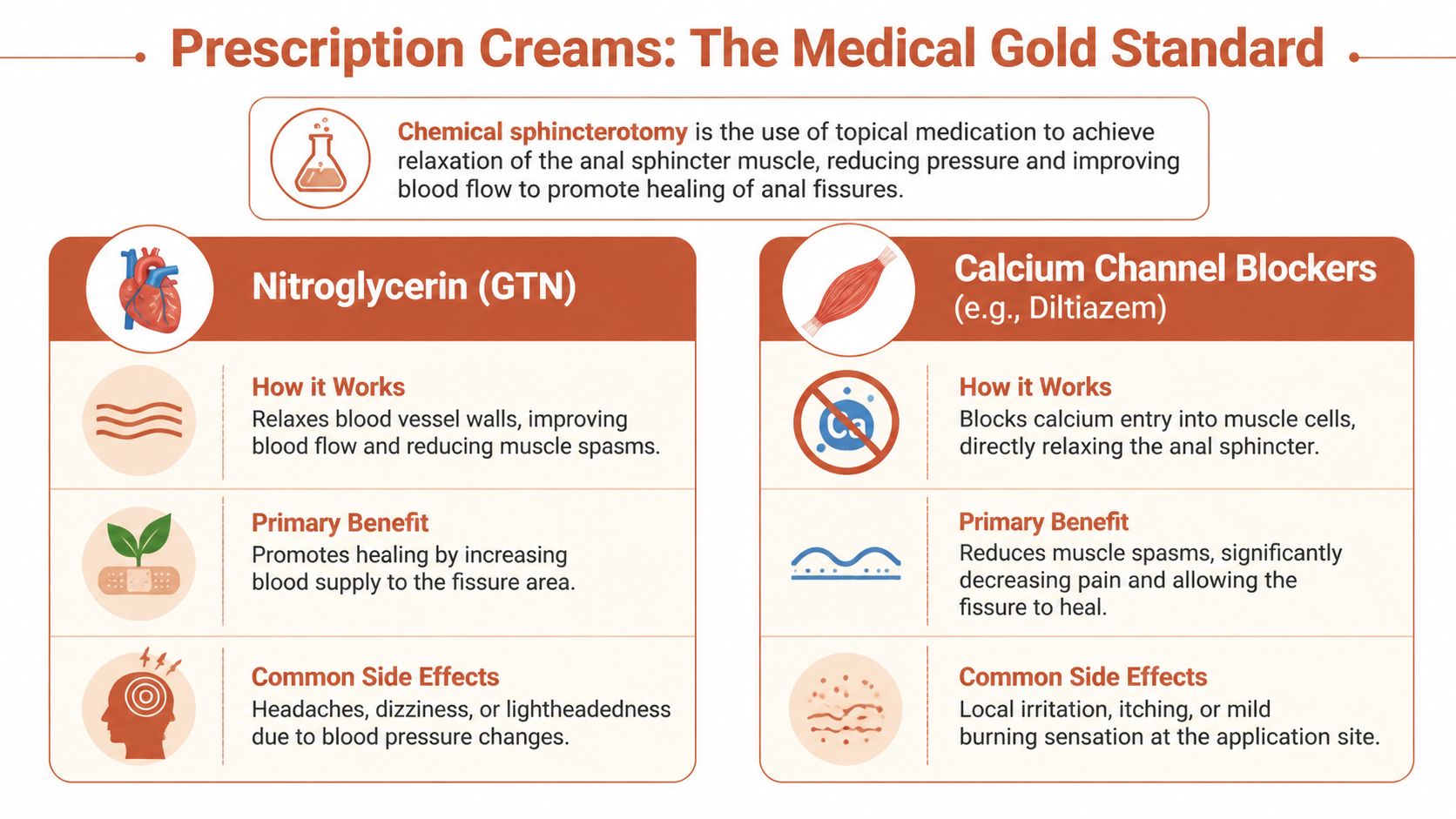
Nitroglycerin and glyceryl trinitrate
Glyceryl trinitrate, also called GTN or nitroglycerin, is one of the oldest prescription options for fissures. It relaxes the internal anal sphincter and improves local blood flow. Those two effects matter because a fissure fails to heal for mechanical reasons, not just because the skin is irritated. Nitroglycerin is the key ingredient found in Bummed's Rapid Relief Hemorrhoid & Fissure Rx Cream.
Nitroglycerin works, but the trade-off is familiar in clinic. Headaches are common enough that some patients stop using it before the fissure has had time to close. A medicine only helps if a patient can stay on it long enough and use it consistently.
Calcium channel blockers
Topical diltiazem and nifedipine are often preferred because they target the same sphincter spasm with fewer headaches for many patients. Diltiazem is the key ingredient in Bummed's Long-Acting Hemorrhoid & Fissure Rx Cream, while nifedipine is the key ingredient in Bummed's Sensitive Care Hemorrhoid & Fissure Rx Cream. They reduce calcium entry into smooth muscle cells, which lowers resting sphincter tone. Lower tone means less squeezing of the wound and better blood supply to the tissue trying to repair itself.
A review in the Canadian Family Physician summary of topical treatments for anal fissure found that calcium channel blockers produced higher healing rates than control treatment in the studies reviewed, and caused fewer headaches than nitroglycerin in head-to-head comparisons.
That balance often matters more than small differences on paper.
Nifedipine versus diltiazem
Both are reasonable prescription choices. The better option depends on side effects, local compounding availability, cost, and how sensitive the patient is to irritation or headache.
Topical nifedipine is commonly compounded for fissure treatment and is discussed in more detail in this guide to nifedipine for healing anal fissures. Diltiazem is also widely used and can be a good choice when clinicians want a muscle relaxant with a track record of tolerability.
From a treatment standpoint, the key point is not which name sounds more familiar. The key point is that both address the reason the fissure is stuck. They relax the internal sphincter, lower pressure, and give the tear a better healing environment.
For many adults, a calcium channel blocker is the best cream for anus fissure because it targets sphincter spasm and is often easier to tolerate than nitroglycerin.
What compounded prescriptions add
Compounded fissure creams give clinicians flexibility that off-the-shelf products do not. The active drug, strength, and base can be adjusted based on the patient’s symptoms and side-effect history. That matters in real practice. A patient with severe spasm, a patient who develops nitrate headaches, and a patient with recurrent fissures may not do best with the same formula.
Bummed is the only telehealth option that offers provider-reviewed prescription fissure creams using ingredients such as nitroglycerin or diltiazem when appropriate. The important point is the treatment category. Prescription fissure creams can succeed where OTC products fail because they are built to reduce sphincter pressure and improve blood flow, which is what the fissure needs in order to heal.
Proper Application and Lifestyle Changes for Healing
A good fissure cream can fail if it’s used inconsistently, applied in the wrong place, or paired with a bowel pattern that keeps re-tearing the tissue. Healing comes from the combination of the medication and the daily habits around it.
How to apply fissure cream properly
Most prescription fissure creams work best when placed just inside the anus, where the internal sphincter sits. Smearing medication only on the outside skin often misses the target.
A simple routine usually works best:
Wash gently first: Use water and pat dry. Avoid aggressive wiping.
Use a small amount: A pea-sized amount is often enough unless your provider instructs otherwise.
Apply just inside the opening: The goal is the sphincter, not deep insertion.
Wash your hands after application: This is especially important with nitroglycerin.
If you want a visual walk-through, our guide on how to put hemorrhoid cream exactly where you need it covers a technique that also helps many adults using fissure medication.
The bowel regimen matters as much as the cream
A fissure won’t heal well if every bowel movement is traumatic. The target is a soft, formed stool.
Helpful habits include:
Fiber intake: Aim for 25 to 35 grams daily from food, supplements, or both.
Hydration: Fiber without enough fluid can backfire.
Osmotic stool support: Polyethylene glycol or magnesium can help some adults keep stool soft.
Short toilet time: Don’t sit and strain. Don’t scroll on your phone.
Less caffeine if it worsens symptoms: Some people notice more irritation or dehydration.
Warm baths and pressure reduction
Warm baths help because warmth relaxes the sphincter. For many people, a short soak after bowel movements reduces that post-bathroom spasm that makes fissures linger.
Also pay attention to pressure and friction through the day:
Avoid prolonged sitting when possible.
Don’t delay bowel movements if you feel the urge.
Wipe less, rinse more if the area is raw.
A fissure cream is not a stand-alone fix. It works best when the stool is soft, the muscle is relaxing, and the area isn’t getting re-injured every day.
Pain control can also help break the guarding cycle. Acetaminophen or ibuprofen can be useful for some adults, and topical lidocaine may help, though it can sting or irritate in some people.
Your Healing Timeline and What to Expect
A common pattern in clinic goes like this. The first week is miserable, the second week feels a little better, and by that point many patients assume the fissure is healed. Then they stop the cream, have one harder bowel movement, the internal sphincter clamps down again, and the tear reopens.
That is the part many people do not expect. Pain often improves before the fissure has closed.
What usually improves first
The earliest change is usually less post-bowel-movement spasm. Bowel movements may still sting, but the pain often fades faster and the hours-long ache becomes less intense. That matters because it tells you the muscle is starting to relax, which improves blood flow to the fissure.
Healing of the skin lining takes longer. A fissure is not like a simple paper cut on the hand. It sits in an area that stretches, contracts, and gets exposed to friction every day. If treatment is stopped as soon as the pain eases, the cycle of spasm and re-tearing can start again.
A realistic treatment window
Most adults should expect a course measured in weeks. Some notice early symptom relief within the first couple of weeks, but stable healing commonly takes 6 to 8 weeks, sometimes longer if the fissure is chronic or constipation remains in the picture.
That timeline makes physiologic sense. The medication has to keep the internal sphincter relaxed long enough for blood flow to improve, inflammation to settle, and the split in the lining to seal without being pulled open again. If you want a broader overview of how that fits into the full treatment plan for an anal fissure, it helps to see creams as one part of a stepwise strategy, not a stand-alone fix.
A practical way to judge progress is by function, not just pain.
| Stage | What you may notice |
|---|---|
| Early treatment | Shorter spasms after bowel movements, less burning, less dread before toileting |
| Mid-course | Bowel movements pass with less resistance, bleeding becomes less frequent, soreness no longer dominates the day |
| Late course | Symptoms stay controlled between bowel movements, and the fissure is less likely to re-tear with minor stool changes |
Side effects and special situations
Nitroglycerin commonly causes headache or lightheadedness. In practice, that is one of the main reasons patients stop using it. Diltiazem or nifedipine are often easier to stay on, even though they still need consistent use to work.
Constipation from GLP-1 medications, iron, opioid pain medicine, or dehydration can slow healing even when the prescription cream is appropriate. In those cases, the cream is not failing. The fissure keeps getting mechanically stressed.
Pregnancy also changes the decision-making. Some topical options may still be reasonable, including compounded formulations in selected cases, but the choice should be individualized with a clinician who knows your symptoms, trimester, and medication list. Bummed's Long-Acting Hemorrhoid & Fissure Rx Cream and Sensitive Care Hemorrhoid & FIssure Rx Creams are generally pregnancy-safe, but should still be reviewed with your provider.
When to Escalate Care Beyond Topical Creams
A common turning point is this: the pain is better for a few days, then one bowel movement sets everything off again. That pattern usually means the fissure is still active beneath the surface. The skin has not fully healed, or the internal sphincter remains too tight for the area to get the blood flow it needs.

When medical therapy has probably run its course
Escalation makes sense after a proper trial of treatment. In practice, that means you used a prescription muscle-relaxing cream as directed, kept stools soft, avoided repeated straining, and still have ongoing pain, bleeding, or frequent re-tearing after several weeks.
Chronic fissures behave differently from fresh tears. Once scar tissue forms, a sentinel skin tag appears, or the exposed muscle fibers stay in spasm, the fissure often gets stuck in a cycle that topical care alone may not break.
Persistent severe pain also deserves a closer look because not every painful anal condition is a fissure.
The next steps providers commonly use
Treatment usually advances in a stepwise way based on how long the fissure has been present, how much spasm is driving symptoms, and whether the exam shows chronic changes.
Botulinum toxin injection into the internal sphincter: This relaxes the muscle for a limited time and can give the fissure a chance to heal.
Lateral internal sphincterotomy: This is the operation with the strongest track record for chronic fissures that have not responded to medical treatment.
Re-evaluation of the diagnosis: If the pattern is atypical, a clinician may look for hemorrhoids, an abscess, Crohn’s disease, infection, or another cause of anal pain and bleeding.
Botox is a reasonable middle step for many adults who want to avoid surgery or are not ideal surgical candidates. Sphincterotomy works well, but it is still surgery, so the decision should weigh healing rates against the small but real risk of changes in continence.
Why a proper topical trial still matters
The goal is not to keep using cream indefinitely. The goal is to give the fissure a fair chance to heal before moving to a procedure.
Prescription creams target the mechanism that keeps chronic fissures open. They reduce internal sphincter tone, improve blood flow, and lower the repeated tension that splits the wound back open. If that mechanism is still active after a full course, more of the same cream is less likely to change the outcome. At that point, stepping up care is medically sensible.
If you want to see how this fits into the full stepwise treatment plan for anal fissure, it helps to compare creams, Botox, and surgery based on where healing is getting stuck.
A good rule is simple. Escalate when symptoms stay active despite correct medication use and stool management, or when the diagnosis itself is no longer clear.
Frequently Asked Questions About Anus Fissure Creams
What is the best cream for anus fissure
Usually, it’s a prescription cream with a smooth muscle relaxant, such as nitroglycerin, diltiazem, or nifedipine. The best choice depends on whether you tolerate headaches, how chronic the fissure is, and whether constipation is still driving repeated injury.
Can lidocaine heal a fissure
No. Lidocaine can reduce pain, which may make bowel movements easier, but it doesn’t fix the underlying spasm and reduced blood flow that keep chronic fissures from healing.
How long should I use fissure cream
Use it exactly as your provider prescribes. Many adults need a full course over several weeks. Stopping once the pain improves, but before the tissue has healed, is one of the most common reasons fissures come back.
Is hydrocortisone good for anal fissures
It may calm irritation, but it usually isn’t the main healing treatment for a fissure. Fissures typically need a medication that relaxes the internal sphincter.
What if the cream burns when I apply it
A mild sensation can happen with some medications, but ongoing burning, rash, worsening pain, or severe headache should prompt a message to your provider. Sometimes a different active ingredient or base works better.
When should I worry that it’s not just a fissure
Seek medical evaluation if you have persistent bleeding, severe pain that isn’t improving, drainage, fever, a lump that’s changing, or symptoms that keep returning despite appropriate treatment. Not every anorectal pain problem is a fissure.
If you’re dealing with ongoing fissure pain and over-the-counter products haven’t worked, Bummed offers a provider-reviewed telehealth pathway for prescription anorectal treatments, including fissure-focused compounded creams when appropriate.
Bummed content is for general education and should never replace professional medical advice that considers your individual health. If you think you’re experiencing a medical emergency, call 911 or head to the nearest emergency department.
Prescription products require an online consultation with a physician who will determine if a prescription is appropriate.